Research
Debunking and Pseudoscience, what is it and why?

Debunking the ‘Pseudoscience’ Debunkers by Phil Mollon, PhD
Mollon, P. Clinical Psychology Forum. [Division of Clinical Psychology. British Psychological Society] 174. June 2007. 13-16.
[Summary: The writings of those who claim to debunk pseudoscience may themselves be unscientific and can be used oppressively in debates within clinical psychology and the NHS.]
Recent years have seen the emergence of a niche academic genre of ‘pseudoscience debunking’. This features the writings of clinical (often American) psychologists, who see themselves as mounting a campaign to rid clinical psychology, and the therapy world generally, of assumptions, theories, and techniques that this group regard as lacking in scientific validity (e.g. Lilienfeld, Lynn, & Lohr, 2003). I offer some comments on this book and upon two papers recently cited within one NHS Trust in an attempt to restrict the range of psychological therapies available. Throughout the profession’s history, there have been psychologists who attempt to establish their territory and authority, defining what is and what is not allowed within the field, and what methods of enquiry and critical thought are permitted. For example, Hans Eysenck, the original ‘debunker’, writing in 1949 about training in clinical psychology, declared that “therapy is something essentially alien to clinical psychology … we must be careful not to let social need interfere with scientific requirements” [p 173]. Unfortunately, the writings within this new genre of debunkers are themselves often lacking in a genuinely scientific outlook. These become potentially problematic when used to buttress arguments about what kinds of therapy should, or should not, be allowed within the NHS in Britain.
Alleged criteria for pseudoscience
In the opening chapter of their edited collection, Lilienfeld, Lynn & Lohr (2003) state: “One of the major goals of this book is to distinguish scientific from pseudoscientific claims in clinical psychology. To accomplish this goal, however, we must first delineate the principal differences between scientific and pseudoscientific research programs.” [p 5]. Clearly they are here stating an agenda of delineating territory and its boundaries. They then go on to propose a list of 10 indicators of ‘pseudoscience’. These are:
- An overuse of ad hoc hypotheses designed to immunise claims from falsification – where hypotheses are ‘pasted on’ to plug holes in the theory;
- An absence of self-correction, with resulting intellectual stagnation;
- Evasion of peer review;
- Emphasis on confirmation rather than refutation;
- Reversed burden of proof – demanding the sceptics demonstrate that a claim is false;
- Absence of connectivity to other scientific disciplines;
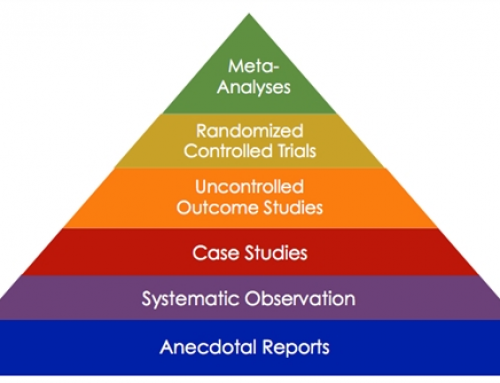
- Over-reliance on testimonial and anecdotal evidence;
- Use of obscurantist language;
- Absence of boundary conditions – i.e. claims that a treatment method has a very wide range of applications;
- The ‘mantra of holism’ – that phenomena are not to be studied in isolation from other phenomena.
The problem with most of these criteria is that they depend somewhat on which pot wishes to call which kettle black. For example, with regard to ‘obscurantist language’, some of the most inelegant and jargonistic language is found in the cognitive-behavioral literature – where facing your fears is called ‘exposure’, refraining from an activity is called ‘response prevention’, learning to relax is called ‘stress inoculation’, and revising your thoughts is called ‘cognitive restructuring’. Beck’s cognitive therapy not only lacks ‘connectivity’ to psychological findings regarding cognition and mood, but is incongruent with it (Fancher 1995). As for ‘boundary conditions’, CBT seems to be prescribed for almost everything these days, from chronic pain to schizophrenia. Any novel theory or therapeutic approach, particularly of a holistic nature, is likely to be dismissed as pseudoscience on the basis of the above criteria. Case studies are always likely to be initial forms of evidence – and, indeed, in many instances are the most appropriate kind of data [Roth & Fonagy, 1996, p 16-17]. Although the principle of falsification is important, it is not unreasonable also to cite evidence that is consistent with the theory in question – confirmatory evidence is surely not irrelevant (Stove 1982). Any radically new approach is likely to display a relative lack of connection to the dominant paradigm, but may have connections to more distant fields of scientific enquiry. A new approach may also not yet have access to established journals willing to consider papers that derive from an unfamiliar paradigm. If a manuscript is sent to reviewers who are invested in a prevailing paradigm they may be likely to reject it. Therefore it is often the case that new approaches are presented first in the form of books, with case histories – as with early accounts of behavior therapy and cognitive therapy, and some of the recent therapies, such as Eye Movement Desensitization, Thought Field Therapy, and so on.
Creating a negative impression
There are certain common styles and strategies that can be discerned in the writings of the debunkers – one obvious feature of which is the use of disparaging terms such as ‘pseudoscience’ and ‘junk science’, as well as a tone of writing that can appear distinctly sneering. This distortion of genuine scientific enquiry has been carefully explored by Perkins and Rouanzoin (2002) in relation to EMDR – and is also discussed in Mollon (2005).
For example, Gaudiano & Herbert (2000) refer to various new psychological therapies (such as Eye Movement Desensitization [EMDR] and Thought Field Therapy [TFT]), stating “these treatments are gaining widespread acceptance among mental health practitioners despite their frankly bizarre theories and absence of scientific support” (p 1 of internet version) – an introduction clearly designed to evoke a negative impression in the reader. Then, referring to EMDR, they write that this “involves a therapist waving his or her finger in front of the patient’s eyes while the client imagines various disturbing scenes that are thought to be related to the patient’s problems” [p 1]. Note the subtle disparaging phrasing here: rather than simply say that the client thinks of his or her traumatic memories, the authors write in a way that implies some speculative theory about the relationship of ‘disturbing scenes’ to the ‘patient’s problems’, when in fact the disturbing scenes are the patient’s presenting problem.
In a similar paper, Devilly (2005) engages in disdainful comments about a number of new therapies. For example, he introduces Traumatic Incident Reduction by describing it as “a direct conversion from Scientology” [438] – an allusion presumably designed to create a negative emotional impression in the reader. He cites no evidence for this claim – and it is at odds with the TIR Association website, where its originator states the background influences as predominantly Freud, Pavlov, Carl Rogers, and cognitive therapy. The method is in essence to do with allowing the client to review a traumatic incident from a position of safety and relaxation – and it is puzzling why this should be regarded as either unusual or controversial.
The sleight of hand style of misrepresentation continues when Devilly refers to a randomized control trial of Emotional Freedom Technique (a derivative of TFT). Whilst acknowledging that the results displayed a significant treatment effect of EFT, he then claims that “at follow-up treatment gains had dissipated to a large extent” [438]. What the paper actually states is more or less the precise opposite: “This immediate effect of EFT appears to be long-lasting. This is especially clear in terms of improvement in avoidance behavior. For BAT (the behavioural avoidance test), the evidence was clear-cut; the follow-up showed (a) substantial improvement compared to the pretest and (b) no evidence of dissipation relative to the posttest. … Thus, converging evidence from four interrelated sources leads to the same conclusion, namely that on the important behavioral task, EFT produces an effect which lasts at least six to nine months.” [Wells et al. 2003. p 956].
Disparagement of motives
Devilly, like others writing in this genre, engages in extensive disparagement of the motives and integrity of those who develop the newer therapies. For example, in referring to Thought Field Therapy, Emotional Freedom Techniques, and EMDR, he makes various statements about how much trainings may cost. The implication appears to be that such methods are essentially a means of conning practitioners and the public out of their money.
Then, in referring to what he alleges to be a kind of manufactured sincerity, he remarks: “… it is even harder to argue with someone who is seen as ‘gifted’ and affects ostentatious compassion towards those in strife. Maybe they set up a ‘humanitarian’ (and tax exempt) offshoot, such as the EMDR Humanitarian Assistance Program, or maybe all they do is sign all correspondence with the word ‘hugs’ instead of ‘yours sincerely’, as in the case of the founder of EFT.” [441]
Presenting theory without acknowledging it as theory.
Devilly makes much of scientific method based on the presentation of falsifiable hypotheses, even quoting Popper to remind the reader of this principle. He states that the major difference between science and pseudoscience is “that empirically supported practices build upon a scientific theory and state the terms under which this theory could be falsified.” [443]
Devilly then goes on to present a broad social psychological theory to answer the question “how did these interventions obtain such a widespread following of practitioners?”. Disregarding the more obvious and simpler hypothesis that the methods become popular because people find that they work very well, he proposes a theory of the “social influence strategies … commonly used by those peddling pseudoscience,” involving speculative hypotheses about the mental processes of the developers and practitioners of the newer methods. An example of Devilly’s hypothesizing is as follows. It concerns the thought processes that might lead a psychiatrist to take a further level of training in a particular method, having already attended an introduction: “In effect, the target (e.g. psychiatrist) rationalizes that they must be interested as they have already invested substantial time and money into the practice. It is also no accident that these trainings are held at plush, five star hotels, which convey a sense of credibility whilst at the same time pairing a positive affect with the technique.” [440]
He devotes more or less 4 pages to outlining this theory – but presenting it as if it were a simple description of social reality. Despite his own emphasis upon falsification, it is actually difficult to see how his theory – with its many embedded assumptions and hypotheses about motives, thought processes, and mechanisms of defence – could be disproved. Whilst appearing cautious and scientific at one moment, when criticizing the studies published by practitioners of methods he does not like, at other moments Devilly presents wildly speculative and sweeping generalizations about large-scale social phenomena.
The kind of writing and reasoning found in Devilly’s paper, and others of its genre, may be regarded as journalistic rather than embodying genuine scientific enquiry. It may create a superficially plausible impression, but is not actually helpful in fostering a thoughtful enquiry into the inherent ambiguity and complexity of clinical phenomena and their treatment.
Rhetorical strategies of debunking
The following rhetorical strategies seem common in the ‘debunking’ literature:
- A subtle misrepresentation of the target – seemingly designed to create in the reader a negative impression of the target.
- Comments that appear designed to disparage the motivations of the developers of the target approach.
- Citing research in such a way, through subtle distortion and selective attention to detail, as to imply that it provides scant support for the target method.
- The selective citation of references so as to support the author’s narrative.
- Seemingly cautious attention to scientific detail and methodology at certain points is combined with sweeping and unsubstantiated generalizations at other points.
- Presenting a theory (or theories, or sets of hypotheses) regarding [a] the mode of action of a therapeutic method, [b] the appeal of the method to its practitioners (including their motives and cognitive-emotional processes), and [c] the motives and mental processes of the developers or promoters of the method – but without making clear that these are hypotheses or theories.
- A dogmatic assertion of what is and what is not to be termed ‘science’.
The common factor running through these features is prejudice – an aggressive assertion of ‘knowing already’ without the humbling necessity to find out. This state of believing oneself to know already is, I suggest, a profound obstacle to free thought and enquiry. When it is harnessed to political and economic pressures towards degraded and depleted versions of cognitive-behavioral therapy, under the guise of ‘evidence-based practice’, the outlook for the once vibrant and unruly creativity of clinical psychology could be bleak indeed.
References
Devilly, G.J. 2005. Power therapies and possible threats to the science of psychology and psychiatry. Australian and New Zealand Journal of Psychiatry. 39 [6] 437-445.
Eysenck, H.J. 1949. Training in clinical psychology. An English point of view. American Psychologist. 4. 173-177.
Fancher, R. 1995. Cultures of Healing. Correcting the Image of American Mental Health Care. New York. Freeman.
Gaudiano, B.A., & Herbert, J.D. 2000. Can we really tap our problems away? A critical analysis of thought field therapy. Skeptical Inquirer. July/August.
http://www.csicop.org/si/2000-07/thought-field-therapy.html
Lilienfeld, S.O., Lynn, S.J., & Lohur, J. 2003. Science and Pseudoscience in Clinical Psychology. New York. Guilford.
Mollon, P. 2005. EMDR and the Energy Therapies. Psychoanalytic Perspectives. London. Karnac.
Perkins, B.R., & Rouanzoin, C.C. (2002) A critical evaluation of current views regarding eye movement desensitization and reprocessing (EMDR); clarifying points of confusion. Journal of Clinical Psychology. 58. [1]. 77-97.
Roth, A., & Fonagy, P. 1996. What Works for Whom? London. Guilford.
Stove, O.C. 1982. Popper and After. Four Modern Irrationalists. New York. Pergamon Press.
Wells, S., Polglase, K., Andrews, H.B., Carrington, P.,& Baker, A.H. 2003. Evaluation of a meridian based intervention, emotional freedom techniques (EFT) for reducing specific phobias of small animals. Journal of Clinical Psychology. 59. 943-966.
Phil Mollon PhD.
Psychoanalyst and Psychotherapist,
Head of Psychology and Psychotherapy Services,
Mental Health Unit,
Lister Hospital,
Stevenage,
Herts.
SG1 4AB
Photo: Natasha Connell on Unsplash